Rural areas are especially vulnerable areas due to the distance of various health resources, including hospitals. The picture above is from a brunch I went to back in August 2004, when I was discussing about rural health issues with my colleagues, during my time in Augusta, GA. Dr. Cook, pictured in the middle, currently has his own eye institute and works as an ophthalmologist, performing 1,000 surgeries per year. I have family that I have lost due to the fact that it was too late to get to the nearest hospital after experiencing an arrhythmia that turned fatal as well. I have heard of stories-all too familiar-that the connectedness they feel in the city, they no longer feel in rural areas due to the sparseness and distance of resources. Unwrapping the complexity requires a specific lens.
I remember spending my early days in rural South Carolina interviewing about how a local paper factory had laid off people, and now they not only had to deal with the effects of the noxious chemicals that I smelled in the air but also the occupational strain of being unemployment. I spent time working with rural doctors and I specifically remember talking to one rural doctor who stated the challenges of having to know everything, placing excessive burden on each healthcare provider. He said that the traditional country doctor was responsible for making house visits, but as times changed, it was important to try to create a medical home for each community resident. This affected the community that people live, work, and play in. I spent some of my early days in conducting secondary data analysis.
I remember going to Philadelphia and listening to wonderful presentations about 7 years ago as part of the National Rural Health Association. One presentation that I worked on was:
A population-based cross-sectional comparison of cardiometabolic syndrome in U.S. rural and non-rural adults
Specifically, I remember the 20th Rural Multiracial and Multicultural Health Conference at Philadelphia, PA. For this conference, myself and other collaborators presented:
Poor mental health and myocardial infarction among African Americans females in rural America: Comparison with rural non-Hispanic Caucasian females
There was a presentation about Native American rural concerns that I remember regarding land rights. This was specifically part of the I have studied rural health in multiple contexts and conducted both primary and secondary studies as well.
Next, in March of 2016, I presented on colon cancer and rural health at Pittsburgh, PA at the American Academy of Family Physicians conference. Specifically, I found that colon cancer screening was lagging behind in rural Pennsylvania.
Gender Disparities in Colon Cancer Screening uptake in Rural Pennsylvania
Rural areas are especially vulnerable due to access gaps. According to the 2014 RUPRI Health Panel report, Access to Rural Health Care - A Literature Review and New Synthesis, barriers to healthcare result in unmet healthcare needs, including a lack of preventive and screening services and treatment of illnesses.
One example-Small Area Income and Poverty Estimates (SAIPE) Program
The U.S. Census Bureau’s Small Area Income and Poverty Estimates program produces single-year estimates of income and poverty for all U.S. states and counties as well as estimates of school-age children in poverty for all 13,000+ school districts.

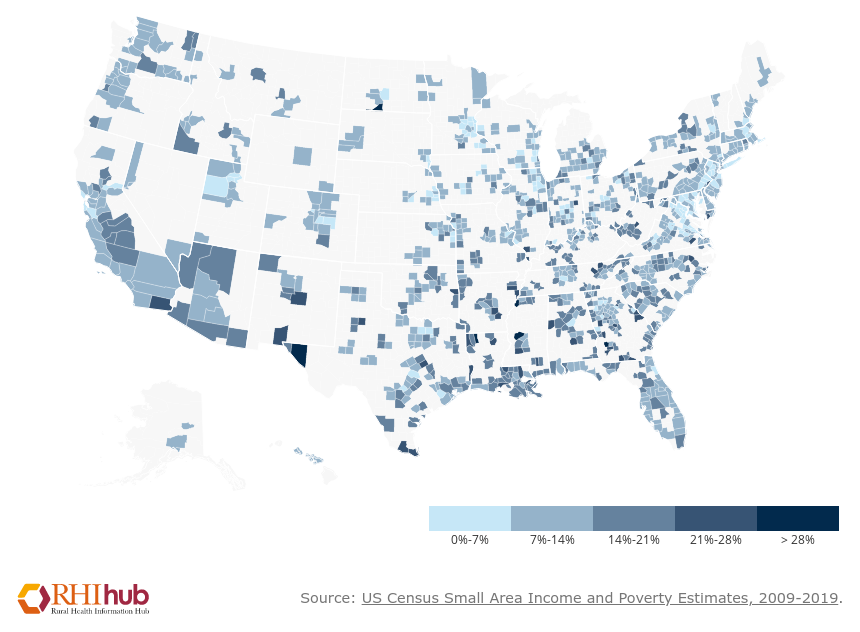
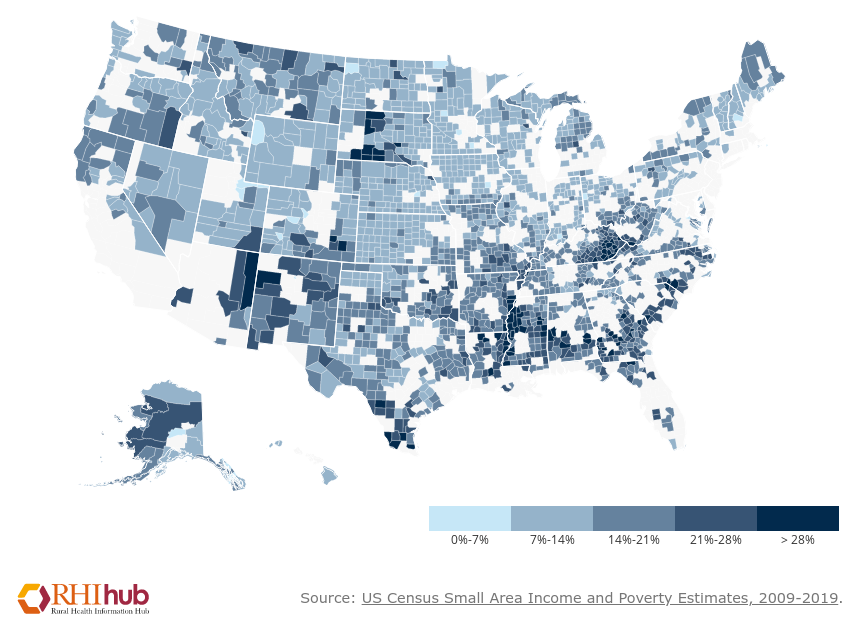
The top picture depicts a map of all of United States. This is a map of over 3000 counties within the United States using Small Area Income and Poverty Estimates-2019. In this Rural Health Information Hub, you can find additional maps. The map on the right is rural and the picture on the left is urban. In both cases, there are areas where there are higher poverty rates. Darker colors are related to resource-poor areas.
Over the years, I have many students who reside in Nigeria. I consider Lagos, Nigeria my second home as many of my collaborators live there. I conducted multiple studies on injury prevention and maternal health. My primary study was a multi-year study that I coordinated in the area of Keffi, Nigeria. Maternal care in rural areas requires more ultrasound care.
I spent some of my early days in conducting secondary data analysis as well.
I remember going to Philadelphia and listening to wonderful presentations about 7 years ago as part of the National Rural Health Association. One presentation that I worked on was:
A population-based cross-sectional comparison of cardiometabolic syndrome in U.S. rural and non-rural adults
Specifically, I remember the 20th Rural Multiracial and Multicultural Health Conference at Philadelphia, PA. For this conference, myself and other collaborators presented:
Poor mental health and myocardial infarction among African Americans females in rural America: Comparison with rural non-Hispanic Caucasian females
There was a presentation about Native American rural concerns that I remember regarding land rights. This was specifically part of the I have studied rural health in multiple contexts and conducted both primary and secondary studies as well.
Next, in March of 2016, I presented on colon cancer and rural health at Pittsburgh, PA at the American Academy of Family Physicians conference. Specifically, I found that colon cancer screening was lagging behind in rural Pennsylvania.
Gender Disparities in Colon Cancer Screening uptake in Rural Pennsylvania
Over the years, I have many students who reside in Nigeria. I consider Lagos, Nigeria my second home as many of my collaborators live there. I conducted multiple studies on injury prevention and maternal health. My primary study was a multi-year study that I coordinated in the area of Keffi, Nigeria. Maternal care in rural areas requires more ultrasound care.



If you would like to go over the other titles and topics that can spark ideas for other research topics. I have also provided a link where you can access the document.
Below is research presented at National Faculty Meeting in June of 2016 regarding rural health. I worked on 2013 BRFSS data to yield results:
Cardiometabolic syndrome (CMS) places an individual at a higher risk of stroke and heart failure. The 2013 Behavior Risk Surveillance System survey, the largest national population-based survey, was used for logistic regression modeling. An effect-modifying relationship was found among women between rural residence and CMS.
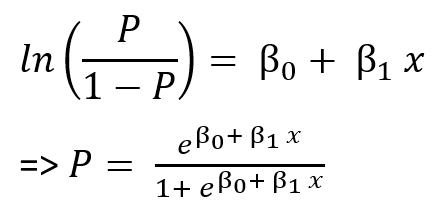
One way to convert some of these equations to prediction scores is to provide a method by which these equations can be created.
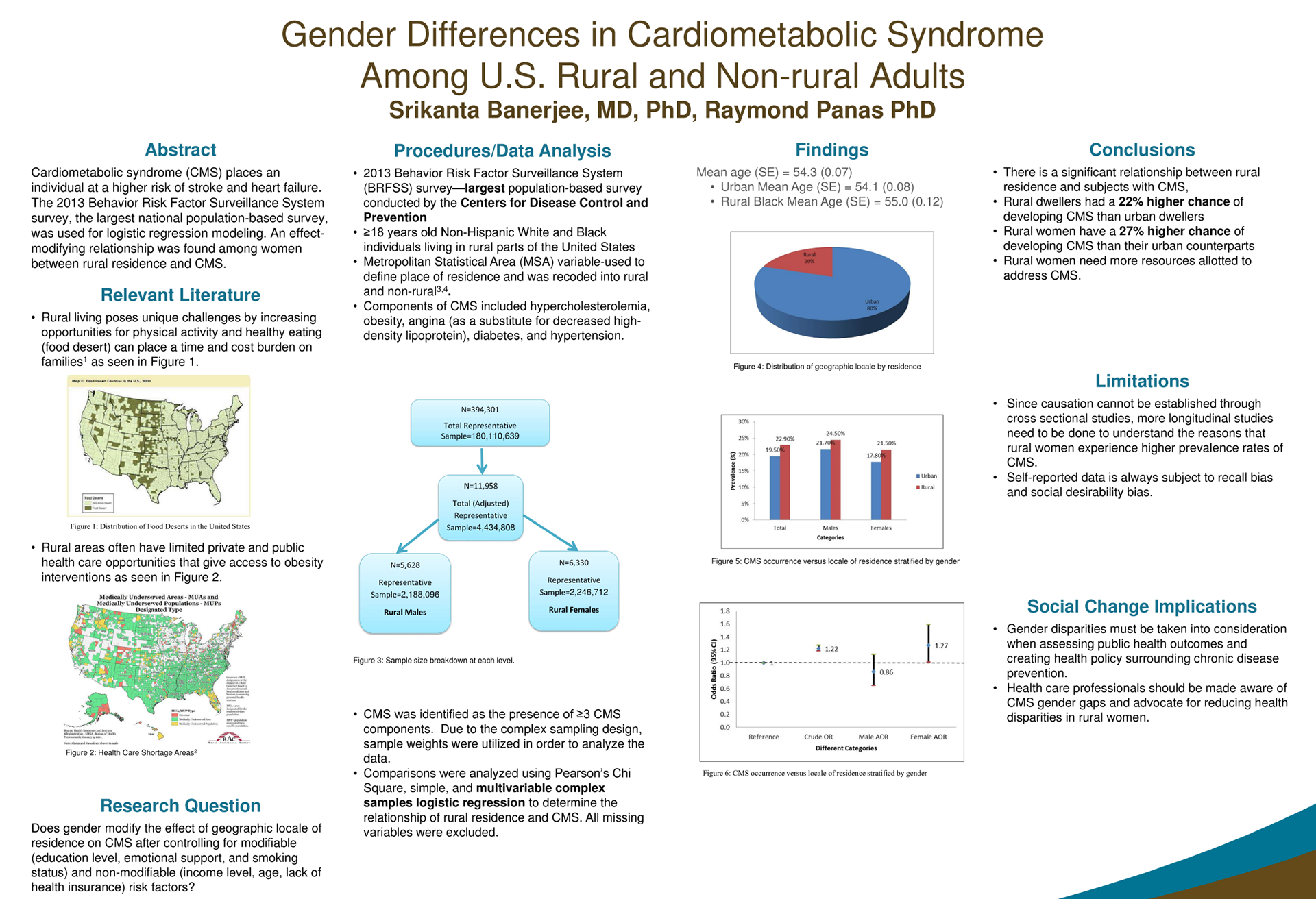
We found rural women having a 27% higher chance of developing CMS than their urban counterparts. In general, rural dwellers were found to have a 22% higher chance of developing CMS than urban dwellers.
One way to understand the strength of a model is by looking at measures like C-statIstic, Akaike Information Criteria, and R-squared (multiple regression). Above is the basic equation for a binary outcome which I will make a video for in the near future. You can find the Scholarworks link.